vaccineregistration.dominica.gov.dm : Covid-19 Pre-vaccine Registration
Organization : Ministry of Health Wellness
Facility/ Service Name : Covid-19 Pre-vaccine Registration
Country : Dominica
Website : https://vaccineregistration.dominica.gov.dm/
| Want to comment on this post? Go to bottom of this page. |
|---|
COVID-19 Pre-vaccine Registration Dominica
Kindly follow the below steps for COVID-19 Pre-vaccine Registration.
How to Register?
Steps :
Step 1 : Visit the official website through provided above.
Step 2 : Read the instructions carefully
Step 3 : Next, click on the “Register for Vaccine” button.
Step 4 : Fill the registration form with the required details
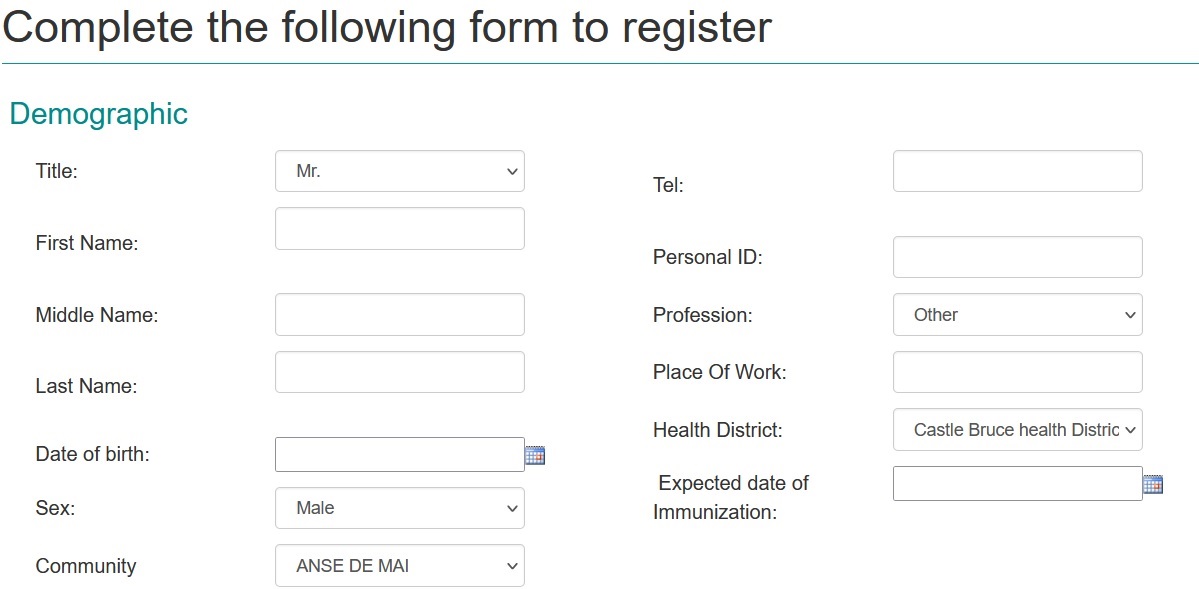
Step 5 : Finally click on the “Submit” button to complete your registration.
Pre-Vaccination Checklist
The following questions will help us determine if there is any reason you should not get the COVID-19 vaccine. If you answer “yes” to any question, it does not necessarily mean you should not be vaccinated. It just means additional questions may be asked. If a question is not clear, please ask your healthcare provider to explain it.
1. Are you feeling sick?
2. Have you ever received a dose of COVID-19 vaccine?
If yes, which vaccine product did you receive?
3. Have you ever had an allergic reaction to: (This would include a severe allergic reaction [e.g., anaphylaxis] that required treatment with epinephrine or EpiPen® or that caused you to go to the hospital.
It would also include an allergic reaction that occurred within 4 hours that caused hives, swelling, or respiratory distress, including wheezing.)
** A component of the COVID-19 vaccine, including polyethylene glycol (PEG), which is found in some medications, such as laxatives and preparations for colonoscopy procedures
** Polysorbate
** A previous dose of COVID-19 vaccine
4. Have you ever had an allergic reaction to another vaccine (other than COVID-19 vaccine) or an injectable medication? (This would include a severe allergic reaction [e.g., anaphylaxis] that required treatment with epinephrine or EpiPen® or that caused you to go to the hospital.
It would also include an allergic reaction that occurred within 4 hours that caused hives, swelling, or respiratory distress, including wheezing.)
5. Have you ever had a severe allergic reaction (e.g., anaphylaxis) to something other than a component of COVID-19 vaccine, polysorbate, or any vaccine or injectable medication? This would include food, pet, environmental, or oral medication allergies.
6. Have you received any vaccine in the last 14 days?
7. Have you ever had a positive test for COVID-19 or has a doctor ever told you that you had COVID-19?
8. Have you received passive antibody therapy (monoclonal antibodies or convalescent serum) as treatment for COVID-19?
9. Do you have a weakened immune system caused by something such as HIV infection or cancer or do you take immunosuppressive drugs or therapies?
10. Do you have a bleeding disorder or are you taking a blood thinner?
11. Are you pregnant or breastfeeding?
12. If pregnant, the stage of pregnancy
13. List if you have any co-morbid conditions or chronic diseases